A Total Knee Replacement surgery is one of the most common surgeries performed today in elderly in view of osteoarthritis and damage to the knee joint.
WHAT IS DONE?
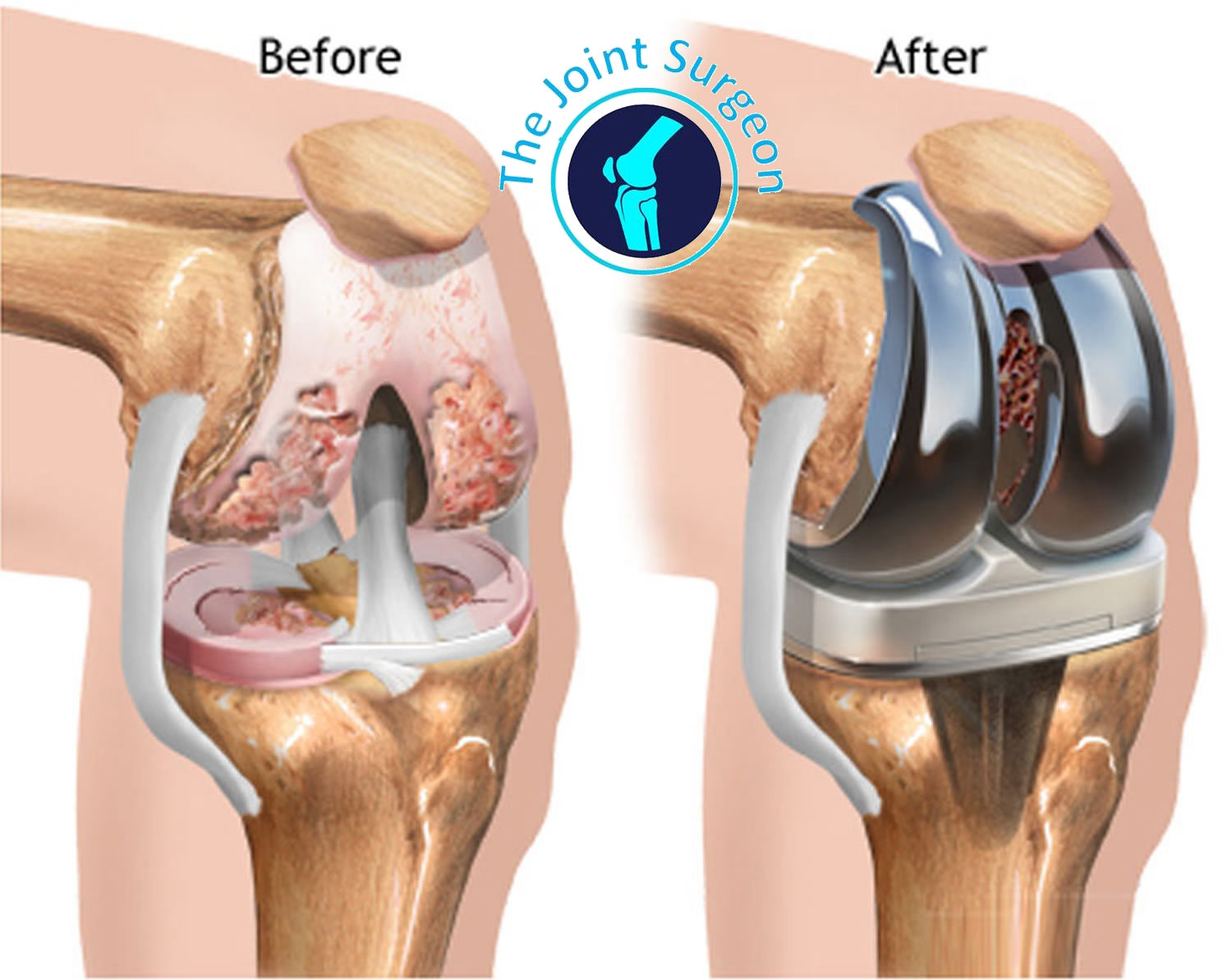
The term knee replacement is a misnomer since the entire joint is not being replaced. Instead, the procedure is more like a knee resurfacing- where only the damaged cartilage and small part of bone near the joint is changed.
The damaged region of the upper and lower bone is removed slightly. The removed cartilage and bones are replaced with metal implants(titanium/cobalt-chromium) that mimic the surface of the joints. The patella might also be resurfaced depending on the surgical necessity. Finally, a medical grade polyethylene spacer for smooth gliding is inserted between the metal components. This completes the process.
The recommendation must always be taken by consulting experts about your specific condition. Some implants are there which can increase knee bending (rotating platform-high flexion) and your surgeon can always consider the feasibility depending on the patient’s clinical profile.
PRE-OPERATIVE STEPS
Every effort is made to assess the patient prior to surgery in order to ensure safety of the patient for the elective procedure.
1. After admission, routine blood work-up will be done prior to surgery. Depending on the age of the patient and other premorbid conditions, other investigations such as Echocardiography may be performed.
2. All the investigations prior to surgery are performed in order to ensure that the surgical procedure can be safely tolerated by the patient, since joint replacement is an elective procedure. If any risk is involved, the patient/ attendants will be informed so.
3. X-rays and/or CT/MRI may be done depending on the surgeon’s choice and the surgical indication for Total Knee replacement.
4. In order to view the alignment of the limb and planning the surgical bone cuts, a CT-scanogram of both limbs is done.
5. Surgical consent will be explained to the patient detailing the procedure as well as the risks involved, if any.
INTRA-OPERATIVE STEPS
Though bone cuts are a major part of the surgery, the key to success of a knee replacement involves the perfect soft tissue (ligament) balancing. The ligaments form a major part of the knee joint and the balance after surgery is of utmost importance.
1. 10-15 cm skin incision is given over the knee joint.
2. The quadriceps muscle is incised. Though the most common approach is medial parapatellar, results are considerably better with mid-vastus* and sub-vastus approach.
3. After Opening the knee joint, bone overgrowths (osteophytes) are removed. The remnants of meniscus, ACL and some amount of patellar fat pad are removed.
4. Depending on the choice of surgeon, PCL may be retained or sacrificed- though both PCL-retaining and PCL sacrificing knee replacements have shown good results.
5. With the help of a jig, the tibial cuts(lower bone) are taken with correct sloping and angle .
6. Similarly the distal femur(upper bone) cuts are taken with correct angle.
7. A spacer is inserted to check the correct space for spacer insertion in extension(knee straightened). If any inequality on inner(medial) and outer(lateral) side is present, soft tissue balancing of Medial structures (superficial and deep MCL) and Lateral structures has to be done.
8. After ensuring the extension gap is correct, Ensuring appropriate rotation femoral-anterior(front), posterior(back) and chamfer(shaping) cuts are done to shape the bone to fit the implant on the femur side.
9. Flexion gap is now checked. The most important is the gap between the bones has to be uniform between the throughout the knee movement in order for a successful knee replacement or else the patient will end up with instability.
10. Once the flexion and extension gap is correctly managed and stable, the remaning bone cuts are taken.
11. Trial components are inserted into place to predict correct positioning and final placement of the actual implant.
12. After thoroughly lavaging the joints with saline the final knee implants are inserted along with cementation (PMMA).
Some surgeons choose to replace patella, but the results with/without replacing patella have been equally good.
POST-OPERATIVE MANAGEMENT
In order to minimize the discomfort and the pain after the surgery, in our center we provide nerve blocks to the patient immediately after surgery so that they do not have to deal with severe pain.
Day 1: Immediately on first day after the surgery, depending on the surgical outcome as well as the patients overall status including bone quality, mobilization- full weight bearing with walker is started. Apart from mobilization, patients are advised to start quadriceps strengthening exercises as well as knee bending.
The patient might experience some amount of pain which should normally subside within 2-4 weeks. There is a chance the surgical wound might soak with blood, though its nothing much to worry about, but its always good to inform your operating surgeon
Day 2-3: On second day, the patient is continued with physiotherapy exercises as on day 1. Along with that the patient is taught on how to ascend/descend the stairs.
Dressing is normally done on day 3 of the surgery.
Day 4-7: The pain reduces from at the time of surgery. If any soakage/discharge from the wound is present, it is always good to inform the operating surgeon.
By this time the patient is normally discharged from the hospital and is advised to continue with home exercises at least twice a day for 10 minutes.
Week 2-6: The pain will substantially reduce for upto 12 weeks as compared to immediately after surgery. The patients should continue the exercises and follow the do’s and don’ts as advised by the operating surgeon.
Sutures are normally removed 15 days after the day of surgery. If there is some gaping in the wound, the surgeon will recall you after 3-7 days for removal of the remaining suture.
After the removal of sutures, wound can be washed with water .Patients should avoid massaging the wound as it may lead to bone overgrowth in soft tissues(heterotopic ossification)which can be problematic later on.
Itching may happen occasionally over the site of surgery. But unless very severe, it can be considered as a part of healing/repair of tissues by the body after surgery
Week 6- 12: A check xray is routinely done at 6 weeks after the surgery in order to see the alignment and fixation. Depending on the condition, most of the patients are advised to reduce from walkers to crutches or walk without support.
DO’S
• You must position your knee comfortably as you go about for your daily activities.
• You should walk and exercise daily. If pain is there, the patient should take medications and continue with exercises instead of avoiding exercises. Exercising post operatively as advised is the key for a good surgical outcome.
• Always use an ice pack for swelling and if pain persists.
• Swelling after a knee replacement surgery though can last for upto 6 months- 1 year, is considered pretty normal. You should elevate your leg one hour twice a day if there is swelling is present. After suture removal crepe bandage can be applied atleast during night time for managing swelling. Though if it is severe, it is always better to show to your surgeon
• You must get trained by your physiotherapist for proper use of walker and cane while walking.
• Always use Western toilets.
DON’TS
• Do not twist your knee.
• Avoid putting unwanted load or stress on your knee.
• Never put a pillow or a roll directly under your knee. Always keep the knee out straight while lying down in bed.
• Avoid sitting in cross leg position or on the floor for at least 12 weeks.
• Avoid driving for 6 to 8 weeks. Start driving only when you are fully recovered and pain free.